Verification of Aided Audibility of Speech
The amount of benefit, or access to speech sounds, a child receives from hearing aids depends on the child's hearing and how audiologists program and verify the hearing aids. The most benefit is achieved when audiologists use real-ear, probe microphone measures to verify hearing aids. Probe microphone verification is a method used to measure the output of the hearing aid, or the amount of speech that is audible, in the child's ear. The aided output can be simulated in a test box or measured directly on the child's ear while they are wearing the hearing aid.
Hearing aid verification should always include speech input, be tested at multiple levels, and take into account the child's individual ear canal acoustics. Speechmapping is one such method that also allows the audiologist to obtain the Speech Intelligibility Index (SII). The SII is highly correlated with the intelligibility of speech and audiologists use it to predict/estimate how much of speech might be understood based on the hearing thresholds, configuration of hearing loss, and output of the amplification. The SII can be measured unaided or aided and results in values between 1 and 100 that describe the proportion of the speech signal that is audible above the hearing thresholds. An SII of 100 indicates full audibility of the speech spectrum, while an SII value of 0 indicates complete inaudibility (none of the speech spectrum is accessible). Read
a discussion on the use of SII in evaluation of hearing aid fittings.
The steps outlined below describe the process of verifying the function of a child's hearing aid using Speechmapping with a real-ear-to-coupler difference (RECD) and simulated real ear response in a test box. Steps 1 and 2 describe the measurement of the RECD (See
"RECD Measurement" for further information on measurement of RECDs in infants and young children). Steps 3 and 4 describe electroacoustic verification of aided speech audibility and advanced hearing aid features.
Step 1: Coupler Response
The measurement of the coupler response is demonstrated in the video below. First, the RECD transducer is coupled to a standard coupler. A signal is introduced via the RECD transducer and SPL as a function of frequency is measured within the coupler.
Step 2: Ear Canal Response
Next, a probe microphone is placed in the ear canal of the child at an appropriate depth (20-25 mm past the intertragal notch). The RECD transducer is connected to a foam tip and inserted into the ear canal alongside the probe microphone. The SPL is then measured in the ear canal of the child. The difference between the responses in the coupler and the child’s ear is then calculated to obtain the RECD. With practice, RECDs can be obtained for most children in a couple minutes per ear. The following video demonstrates measurement of the ear canal response on an 8-month-old child.
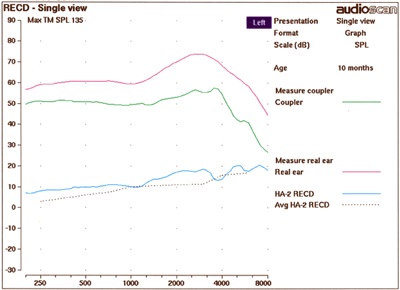
Figure 1. Measured RECD on a 10 month-old. The green line represents the coupler response, the pink line represents the response in the ear canal and the blue line represents the RECD.
Step 3: Verifying Audibility
In infants and small children who are unable to cooperate with in situ (real ear) hearing aid verification, the RECD is used to simulate the real ear response in a test box. The child’s hearing aid is attached to the coupler and microphone in the test box. Speech signals are presented to the hearing aid and output is measured across the frequency spectrum. The test box simulation of a real ear response is shown in the following video.
Figures 2 illustrates the use of soft (50 dB SPL), average (65 dB SPL) and loud (75 dB SPL) speech signals, in addition to a 90 dB SPL signal sweep to test MPO. The output of the hearing aid closely matches the targets prescribed by the fitting formula for the child's hearing thresholds.
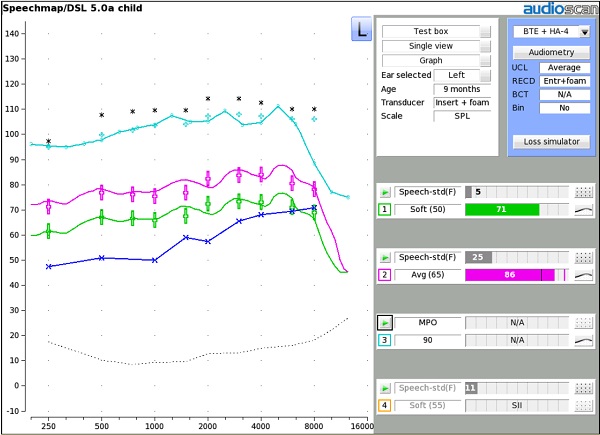
Figure 2. Verifying output of the hearing aid in response to soft (green output) and average (pink output) speech and MPO (light blue output).
The following figure is a comparison of hearing aid output for soft speech for a well-fit hearing aid (pink line) and a poorly-fit hearing aid (green line). Note the difference in SII for the poorly-fit aid (SII=46) and the well-fit aid (SII=72). Matching targets using real-ear, probe microphone verification results in the best match to targets while optimizing audibility of speech.
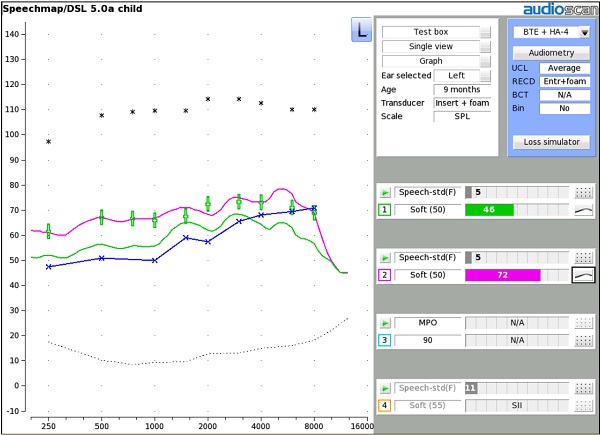
Figure 3. Comparison of a well-fit hearing aid (pink output) to a poorly-fit hearing aid (green output) in response to a soft speech input.
Step 4: Verifying Advanced Features
Modern hearing aids have advanced features aimed at helping improve the audibility of speech, including frequency lowering, digital noise reduction, feedback suppression and directional microphones. Verification of the appropriate function of these features requires extra steps beyond the verification procedure outlined above. To learn more, please see the following links:
Frequency lowering
Here is a
discussion of verification of hearing aids with frequency lowering technology. A frequency lowering verification procedure specific to the Audioscan Verifit can be found on page 61 of the
Verifit User's Guide.
Automatic noise reduction
See Scollie et al. (2016) for a protocol to verify noise reduction features in a child's hearing aid. In addition, a noise reduction verification procedure specific to the Audioscan Verifit can be found on page 112 of the
Verifit User's Guide.
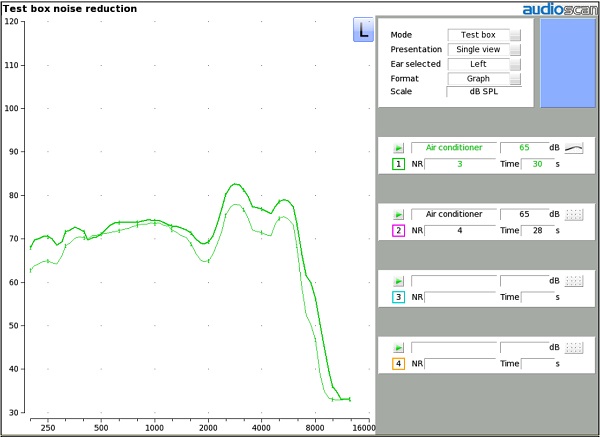
Figure 4. Verification of automatic noise reduction in the test box. The difference between the two hearing aid output curves indicates the amount of noise reduction offered by the hearing aid.
Feedback suppression
A verification procedure specific to the Audioscan Verifit can be found on page 79 of the
User's Guide.
Directional microphones
Here is a
detailed discussion of verification of directional microphones. Audioscan's verification procedure to test functionality of directional microphones can be found on page 113 of the
Verifit User's Guide.
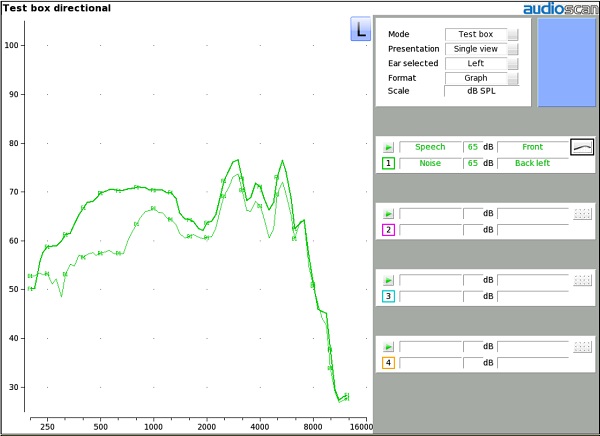
Figure 5. Verification of directional microphones in the test box.
Verification of Bone Conduction Devices
Prescriptive targets and skull simulators are available for clinical verification of bone conduction devices (Hodgetts & Scollie, 2017). Verification systems may have the ability to use a skull simulator and Speechmapping procedures to verify the aided audibility of speech and maximum power output of bone conduction devices. For a specific procedure to verify bone conduction devices, please see page 67 of the
Verifit User's Guide.
Aided Sound Field Testing
Historically, aided sound field and/or functional gain measures were used to verify the adequacy of a hearing aid fitting. These test procedures have numerous shortcomings including the fact that the measures do not provide information about the child's access to speech with the hearing aids and do not test at multiple input levels. Aided thresholds are not sensitive to many of the signal processing differences across hearing aids. Furthermore, maximum output in the ear is unable to be obtained using sound field/functional gain measures. Child state and movement may also impact results. For more information on the limitations of aided sound field testing, see the American Academy of Audiology (AAA) Clinical Practice Guidelines on Pediatric Amplification (2013) and Moodie et al. (2016).
AAA recommends
against the use of aided sound field testing as a verification method of acoustic hearing aids.
References
American Academy of Audiology. (2013).
Clinical Practice Guidelines on Pediatric Amplification. Retrieved from
www.audiology.org.
Moodie, S., Rall, E., Eiten, L., Lindley, G., Gordey, D., Davidson, L., . . . Scollie, S. (2016). Pediatric Audiology in North America: Current Clinical Practice and How It Relates to the American Academy of Audiology Pediatric Amplification Guideline.
Journal of the American Academy of Audiology, 27(3), 166-187. doi:10.3766/jaaa.15064.
Scollie, S., Levy, C., Pourmand, N., Abbasalipour, P., Bagatto, M., Richert, F., . . . Parsa, V. (2016). Fitting Noise Management Signal Processing Applying the American Academy of Audiology Pediatric Amplification Guideline: Verification Protocols.
J Am Acad Audiol, 27(3), 237-251. doi:10.3766/jaaa.15060.