Real-ear-to-coupler difference (RECD) measures take into account a person's unique ear canal or earmold characteristics in comparison to a coupler that simulates an average adult's ear canal. Using RECDs during pediatric hearing aid verification is very important, as infant and young children's ear canals vary significantly in size compared to an adult and the size of children's ear canals regularly change in size as they grow. RECD measurement is quick and can be completed for use in simulated real-ear verification measures in a couple minutes per ear with practice and appropriate distraction for the child.
Although average RECD values do exist for one-month age intervals through the age of 5 years, individual variability of age-related averages is high. Age-related averages do not take into account the unique acoustic characteristics of an individual child's ear or earmold, which can affect the real ear response. The use of age-related average RECD values result in hearing aid fittings matched farther from prescriptive targets compared to a measured RECD (McCreery, Bentler, & Roush, 2013).
Tips for measuring RECDs in children
Prior to RECD Measurement
- Practice on others before making the real measure to increase your comfort level
- Make sure the probe microphone is calibrated prior to the session
- Measure the coupler response before the child's session
- Measure and mark the probe tube with the appropriate insertion depth (10-15 mm from ear canal entrance or 20-25 mm from the intertragal notch)
- Have toys, bubbles or distractors ready before testing starts
Probe-Tube Placement
- During otoscopy, note any wax or drainage that may prevent you from making the RECD measure. Also note the presence of PE tubes, TM perforations, or middle ear effusion, all of which can have an acoustic effect on the RECD
- Determine shape and length of canal before placing probe tube
- Thread the probe tube behind the elastic band before inserting it into the ear canal to keep it from moving after insertion
- Ensure appropriate insertion depth after placing probe tube
In the following video, a probe tube is inserted into the ear canal of an 8-month-old child.
During RECD Measurement
- Use a second examiner or helpful parent to keep the child distracted by playing with toys or blowing bubbles
- Ask the parent to use a least-restrictive hold to limit the child's movements while you insert the probe tube
Note the use of these strategies in the following video.
Troubleshoot Your Measurement
Negative RECD values may result from several sources:
-
Loose-fitting insert earphone or earphone not fully expanded. In this case, low frequency sound leaks out around the earphone leading to negative RECD values in the low frequencies. Make sure the earphone is given enough time to fully expand and consider using a larger insert earphone if needed.
-
Loose-fitting earmold or an earmold with a large vent (if measuring RECD using an earmold). In this case, low-frequency sound leaks out around the canal of the earmold or through the earmold vent. Negative RECD values resulting from venting are most commonly seen below 1000 Hz. Errors in predicted real ear amplified gain may occur with negative RECDs greater than -5 dB, especially when the gain of the hearing instrument is minimal at the same frequencies where the negative RECD values occur. Consider making tighter fitting earmolds for the patient. Measuring the RECD with an earmold with a large vent allows for appropriate gain adjustment taking the ear canal/ear mold acoustics with a large vent into account.
-
Presence of a patent PE tube or TM perforation. The larger ear canal/middle ear volume created by a patent PE tube or TM perforation creates a negative RECD value in the low frequencies. Figure 1 below contrasts the measured RECD values for an intact eardrum (left panel) with an eardrum that has a perforation (right panel). There is no need to re-measure the RECD in cases of a patent PE tube or TM perforation, as it reflects the altered acoustic properties of the larger ear canal/middle ear volume and should be incorporated into the hearing aid fitting. Once the PE tube or TM perforation is no longer present, the RECD will need to be re-measured.
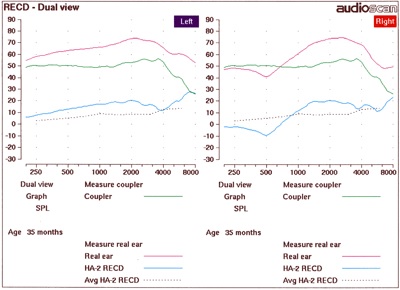
Figure 1. RECD responses for an intact (left panel) versus perforated (right panel) eardrum
-
Shallow probe tube insertions. Negative RECD values may occur in the higher frequencies above 3000 Hz when the probe tube has not been inserted far enough into the ear canal. Figure 2 below illustrates negative high frequency RECD values resulting from shallow probe tube insertion. Remove the probe tube and replace deeper into the ear canal. Verify the new placement using otoscopy.
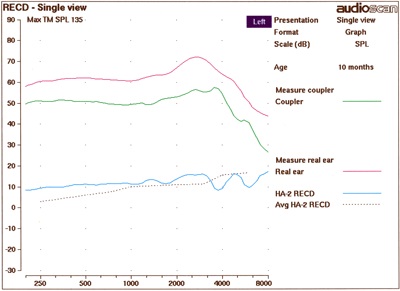
Figure 2. Improper probe tube insertion
-
Blocked probe tube. When RECD values are negative across the frequency range (as seen in Figure 3 below), a blocked or crimped probe tube may be the cause. The tube could be blocked by wax or by incorrect placement of the tube against the ear canal. A tight-fitting earmold can also cause enough pressure to crimp or close the probe tube. Remove and inspect the probe tube for wax impaction before replacing and re-measuring the RECD. You may need to use a new probe tube if the wax cannot be removed from the probe tube. Consider threading the probe tube through the earmold vent if the earmold is crimping the probe tube against the ear canal.
Figure 3. Blocked tube probe
RECD FAQs
Should I use the child's earmold or an insert earphone during RECD measurement?
Ideally, the same coupling method (earmold or insert earphone) will be used both for the assessment of hearing thresholds and the measurement of the RECD. However there are occasions when a mismatch may occur, e.g. insert earphones are used during assessment of audiometric thresholds and then the child's own earmolds are used to measure the RECD. In these cases, the coupling method in each step should be specified within the verification system so that appropriate correction factors may be applied.
See (Moodie et al., 2016) for further discussion on RECDs obtained using a child's personal earmolds.
What if I'm only able to perform an RECD on one ear?
Between-ear RECD values are highly correlated (Tharpe, Sladen, Huta, & McKinley Rothpletz, 2001). The measured RECD from one ear can be used to predict the second ear RECD, unless an obvious difference between ears is found (Munro & Howlin, 2010). If an ear malformation, middle ear effusion, or TM perforation is present, then neither an RECD from the contralateral ear nor an age-related average RECD should be used. In the case of obvious differences between ears, an RECD must be measured for each ear.
What if I'm not able to perform an RECD on either ear?
It is always recommended to measure an RECD for at least one ear. However, using age-related average values is better than ignoring the RECD completely or using aided sound field testing which provides no estimate of output or audibility.
What about middle-ear disease?
Middle ear effusion and tympanic membrane perforations are the most common middle ear conditions that affect the RECD response. TM perforations were discussed above, with the effect being a negative RECD value in the low to mid frequency range. On the other hand, middle ear effusion with increased stiffness of the TM often creates larger positive RECD values across the frequency range tested (Martin, Westwood, & Bamford, 1996). If the perforation is longstanding, measure and use the RECD values for hearing aid fitting. Similarly, if the middle ear effusion is longstanding, use the RECD values for hearing aid fitting. If it is a temporary condition, you may wait until the middle ear is healthy to measure RECD or use a previously measured RECD from when the ear was healthy for the hearing aid fitting.
How often does the RECD need to be repeated?
The RECD should be repeated whenever there is a change in the ear canal/earmold acoustics. The RECD should also be repeated when new hearing thresholds are measured. Most pediatric guidelines recommend that the RECD be repeated whenever the child receives new earmolds, which in infants may be as often as every 2-3 months when they are growing rapidly. McCreery & Walker (2017) recommend measuring RECD as part of hearing aid verification every three months in the first year of life, then every 6 months up until the age of 3 and annually thereafter in children with no risk factors of progressive hearing loss.
References
Martin, H. C., Westwood, G. F., & Bamford, J. M. (1996). Real ear to coupler differences in children having otitis media with effusion.
Br J Audiol, 30(2), 71-78.
McCreery, R. W., Bentler, R. A., & Roush, P. A. (2013). Characteristics of hearing aid fittings in infants and young children.
Ear Hear, 34(6), 701-710. doi:10.1097/AUD.0b013e31828f1033
McCreery, R. W., & Walker, E. A. (2017). Hearing Aid Verification for Children. In
Pediatric Amplification: Enhancing Auditory Access. San Diego, CA: Plural Publishing.
Moodie, S., Pietrobon, J., Rall, E., Lindley, G., Eiten, L., Gordey, D., . . . Scollie, S. (2016). Using the Real-Ear-to-Coupler Difference within the American Academy of Audiology Pediatric Amplification Guideline: Protocols for Applying and Predicting Earmold RECDs.
J Am Acad Audiol, 27(3), 264-275. doi:10.3766/jaaa.15086
Munro, K. J., & Howlin, E. M. (2010). Comparison of real-ear to coupler difference values in the right and left ear of hearing aid users.
Ear Hear, 31(1), 146-150. doi:10.1097/AUD.0b013e3181b8399b
Tharpe, A. M., Sladen, D., Huta, H. M., & McKinley Rothpletz, A. (2001). Practical considerations of real-ear-to-coupler difference measures in infants.
Am J Audiol, 10(1), 41-49.